DFDF Guide to CMS Models
CMS Models Will Keep Changing. Your Architecture Shouldn't.
A Digital-First, Data-First (DFDF) guide to building a reusable Model Operating System for the CMS and CMMI model portfolio, and how organizations can support new models without rebuilding their core.
By Stacy Fox, Chief Growth Officer
Why this guide exists
Most organizations don't struggle with CMS models because of their strategy. They struggle because every new model forces them to rebuild data pipelines, workflows, reports, and governance from scratch. Teams start over. Vendors pile up. Each transition takes longer than the last. That approach does not scale-especially as CMS accelerates the pace of new models and expands participation across providers, payers, and states.
CMS has been clear about its direction. By 2030, the Innovation Center aims for nearly all Medicare and most Medicaid beneficiaries to be in accountable care relationships, with models that are simpler, more aligned, and more equitable. That goal assumes organizations can add and evolve models without re-platforming every three to five years.
At The Garage, we operate a Model Operating System (MOS) designed for this reality. It provides a reusable operating foundation where new CMS models activate through configuration rather than reinvention. In this environment, CMS policy becomes an input to existing operations-not a disruption that forces teams to rebuild core infrastructure.
This guide connects CMS policy direction to operating reality. It explains what CMS and CMMI are repeatedly asking organizations to do, how those requirements recur across the model portfolio, and what it takes to respond with a durable, model agnostic architecture that evolves without rebuilding core systems each time.
The unifying insight: every CMS model reduces to four operating fundamentals
Strip away the policy language and every CMS model comes down to the same operational questions:
- Attribution & eligibility: Who is in scope, when they are in scope, and why.
- Payment logic: How dollars move, what is at risk, and how reconciliation works.
- Measures & outcomes: How performance is defined, stratified, and reported.
- Workflows & auditability: What must happen day to day, and what must be defendable later.
Policy language changes. Incentives shift. Model names come and go. The operating fundamentals repeat.
A model-agnostic platform does not abstract policy. It absorbs variability by implementing these fundamentals once and reusing them across models.
Interoperability is what makes that reuse real. Attribution, payment, measurement, and workflows only hold up when data moves across systems, organizations, and payers with consistent meaning, traceability, and auditability. Without that foundation, every new CMS model fractures operations and forces teams to rebuild what should already exist.
CMS is already moving in this direction at the policy level through the Universal Foundation of quality measures-reusing a core set of measures across programs to reduce burden and increase alignment. At The Garage, we apply that same universal-foundation concept operationally. Our Model Operating System standardizes attribution, payment, measures, and workflows on interoperable, normalized data so new models activate through configuration, not reconstruction.
These four fundamentals become the shared rails. Each new CMS model rides the same operating system with different rules instead of requiring a new track every time.
The Garage architecture: the Model Operating System
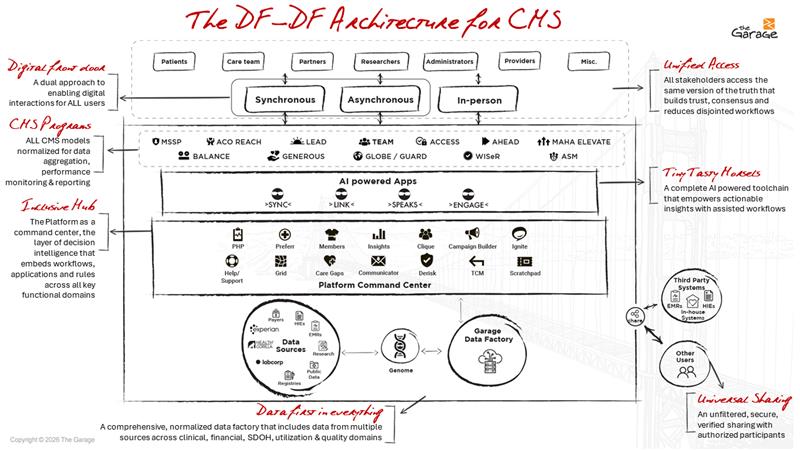
A Model Operating System is the permanent runtime that supports CMS models, present and future. At The Garage, this operating system is grounded in a Digital-First, Data-First (DFDF) architecture:
- Digital workflows come first. What clinicians and staff do every day is captured as structured data, not buried in spreadsheets or side systems.
- Data is normalized, longitudinal, and model-agnostic. Adding LEAD or BALANCE means updating rules, not standing up new pipes.
- AI and automation support operations, not just reporting. Insights help teams decide what to do next, not just what already happened.
- New models activate through configuration rather than custom builds.
Interoperability is treated as a permanent layer, not a one-time integration.
The heavy lift-data ingestion, normalization, identity resolution, interoperability, workflow orchestration, and auditability stays constant across models.
FHIR-based APIs, claims ingestion, event feeds, and partner data are normalized once into a longitudinal, model-agnostic record. New CMS models consume that foundation through configuration, not new interfaces.
This DFDF architecture aligns with CMS's push toward FHIR-based digital quality measures and API-driven interoperability, where standardized data can be reused across models, measures, and programs instead of being rebuilt for each use case.
What Digital-First, Data-First looks like in practice: Care teams work in digital workflows designed for execution. Enrollment, outreach, documentation, and follow-up happen in systems built for action. Data flows automatically into analytics, payment logic, and audit views. Data becomes a byproduct of work, not an afterthought. For example, moving from MSSP to TEAM should not require a new data warehouse, contracting system, and care management tool. It should mean activating episode logic on an existing foundation.
On top of the Model Operating System, The Garage runs:
- Analytics and prediction: Cost and revenue forecasting, risk stratification, episode and readmission risk, equity and leakage analysis, and chronic-care outcome projections. These capabilities help organizations understand what is changing, why it is changing, and where attention is needed.
- AI in daily operations: Agents help teams translate insight into action. It prioritizes outreach, highlights emerging episode risk before discharge, surfaces utilization issues, and brings relevant contract terms into view during reconciliation. The goal is not predicting for its own sake. It is helping people decide what to do next, in the moment.
- Applications: Dashboards and operational consoles for clinicians, finance, pharmacy, and care management. These tools are model-aware, designed for day-to-day execution, and resilient as policy shifts.
The operating system is where repeatable work lives, so teams don't have to reinvent it every time. That is what turns CMS change from an emergency into a manageable release cycle.
This is the difference between implementing a CMS model once and becoming model-ready as CMS and CMMI continue to test, refine, and scale new approaches across the next decade.
The CMS model landscape
Below is a practical overview of the CMS and CMMI model types organizations most often encounter. These examples are illustrative, not exhaustive. The goal is to show that current and future models fall into recognizable operational patterns.
Accountable care and total cost of care
MSSP: ACO accountability for total cost of care and quality; operationally distinct for retrospective attribution, benchmarking, and shared savings and losses.
ACO REACH: Equity-forward accountable care and improved access; operationally distinct for equity stratification, governance rigor, and compliance requirements.
LEAD: Long-horizon accountable care pathways; operationally distinct for stability over time and deeper risk alignment.
Episodes and procedures
TEAM: Mandatory surgical bundles with post-acute accountability; operationally distinct for episode definition, cross-setting coordination, and time-bounded accountability.
Tech-enabled chronic care and state transformation
ACCESS: Outcome-aligned payments for technology-enabled chronic care; operationally distinct for continuous engagement, digital monitoring, and outcome reporting.
AHEAD: State-based multi-payer total cost of care with global budgeting; operationally distinct for cross-payer data integration, geographic attribution, and multi-stakeholder governance.
Prevention and whole-person care
MAHA ELEVATE: Evidence generation for lifestyle and whole-person interventions; operationally distinct for non‑traditional services, patient-reported outcomes, and documentation rigor.
Drug pricing and rebate demonstrations
BALANCE: Access to high-cost therapies paired with lifestyle supports and negotiated pricing; operationally distinct for drug pricing logic with outcomes and adherence tracking.
GENEROUS: Medicaid supplemental rebate structures aligned with international pricing benchmarks; operationally distinct for rebate calculation and contract traceability.
GLOBE / GUARD: International benchmark pricing demonstrations for Part B and Part D drugs; operationally distinct for complex reconciliation and financial audit requirements.
Utilization integrity and specialty accountability
WISeR: Technology-enabled utilization management modernization; operationally distinct for prior authorization workflows, documentation requirements, and compliance visibility.
ASM: Specialist accountability for high-cost conditions such as heart failure and low back pain; operationally distinct for condition-specific attribution and upstream prevention.
How the Model Operating System supports each CMS model
CMS changes the rules. The operating system absorbs complexity. Organizations configure, not rebuild.
Accountable care and total cost of care (MSSP, ACO REACH, LEAD)
What changes: Attribution rules, benchmarks, equity requirements, and governance expectations. What persists: Longitudinal population insight, cost management, quality measurement, and reconciliation discipline.
On a Model Operating System, these models become variations in logic rather than infrastructure. Attribution rules can shift and measures evolve without rebuilding pipelines, care programs, or financial workflows.
Operational implication: Moving between accountable care models becomes a policy transition, not an organizational reset.
Episode-based accountability (TEAM)
Operational reality: Accountability begins at a triggering procedure and continues through post-acute recovery. Episode grouping, time-bounded tracking, partner visibility, and reconciliation activate on top of existing infrastructure. Operational implication: TEAM functions as a new operating mode layered onto existing capabilities.
Tech-enabled chronic care (ACCESS)
Operational reality: Continuous engagement tied directly to outcomes-based payment. Enrollment, monitoring, documentation, and outcome tracking occur inside existing workflows rather than parallel programs. Operational implication: ACCESS becomes embedded in daily operations instead of standing alone as a separate initiative.
State multi-payer transformation (AHEAD)
Operational reality: Population accountability across payers, providers, and geographies. Cross-payer normalization and shared reporting extend the same foundation outward. Operational implication: AHEAD scales capabilities horizontally instead of introducing new systems.
Prevention and whole-person models (MAHA ELEVATE)
Operational reality: Tracking non-traditional services with clinical rigor. Program participation, patient-reported outcomes, and evidence generation operate within governed workflows. Operational implication: Whole-person care gains the same discipline as traditional medical services.
Drug pricing and rebate models (BALANCE, GENEROUS, GLOBE, GUARD)
Operational reality: Complex financial logic with strict traceability. Eligibility, pricing rules, adherence signals, and reconciliation extend existing financial governance. Operational implication: Drug-pricing initiatives integrate into enterprise finance rather than fragment it.
Utilization integrity (WISeR)
Operational reality: Real-time decisions backed by defensible documentation. Eligibility logic, prior authorization workflows, AI-assisted review, and compliance records operate as governed processes. Operational implication: Utilization management becomes a continuous enterprise capability.
Specialty accountability (ASM)
Operational reality: Condition-specific responsibility across care settings. Specialists can see how decisions affect outcomes and total cost across the continuum. Operational implication: Specialty models activate focused accountability without new infrastructure.
How The Garage approaches CMS models
The Garage does not position itself as a "CMS model solution." Our role is not to implement individual programs. It is to make participation in CMS models repeatable, durable, and operationally sane.
We focus on building the operating system that CMS models repeatedly require:
- Interoperable, normalized data
- Digital-first workflows embedded in daily operations
- Configurable analytics and reporting
- Automation and AI that reduce operational burden
- Contract compliance and audit support that withstand scrutiny
These capabilities line up directly with the Innovation Center's strategic objectives to embed equity in every model, streamline the portfolio, and provide tools that support care-delivery transformation, not just new payment methodologies.
When these capabilities are in place, new models do not require new platforms. They require new configurations. That is what allows adoption to accelerate; policy pivots to remain manageable, and scale to stay sustainable.
A simple test for readiness
Whether evaluating MSSP, TEAM, ACCESS, AHEAD, or what comes next, ask four questions:
- Who is in scope?
- How do dollars move?
- How is success measured, for whom and over what time horizon?
- What must be provable, and to whom?
If those answers live in different systems, spreadsheets, or teams, the organization is still implementing models rather than operating them.
If they live in a shared Model Operating System-with configurable rules, shared data, and common workflows, the organization is positioned to keep pace as CMS models consolidate, align, and evolve.
The future belongs to model-ready organizations
The future of value-based care belongs to organizations that invest once, configure often, share data across boundaries, operate digitally by default, and treat policy change as input, not disruption.
CMS models will continue to evolve. Organizations built on durable operating infrastructure will evolve with them.

- I'm curious. I'd like
to set up a demo - What does the
platform do? - Tell me more about
the Garage - What has been the
platform's impact?
